
Postoperative nausea and vomiting
Abstract: Postoperative nausea and vomiting (PONV) remains a significant clinical issue that can detract from patients’ quality of life in hospital/treatment facility, as well as in the days immediately postdischarge. In addition, PONV may increase perioperative costs, increase perioperative morbidity, increase postanesthesia care unit stay, prolong hospital stays, length of stay/delay discharge, delay the time that the patient can go back to work, and lead to readmissions. Despite the existence of multiple tools to stratify patients according to their risk of developing PONV and multiple PONV treatment guidelines, clinicians do not appear to systematically address the treatment and/or prophylaxis of PONV in a uniform fashion with both pharmacologic and nonpharmacologic strategies in attempts to minimize PONV occurrences.
Key words: Postoperative; nausea; vomiting; dopamine receptor antagnosits; NK-1; 5-HT3
Introduction
Over 40 million patients undergo surgery per year in the United States and more than 100,000,000 patients worldwide with about 30% experiencing postoperative nausea and vomiting (PONV) (1). Postoperative nausea and vomiting (PONV) is one of the most commonly reported adverse effects of anesthesia. Even patients with zero known risk factors carry a 10% risk of PONV. This risk increases dramatically to 61% and 79%, respectively, when 3 or 4 risk factors exist (female gender, nonsmoker, history of motion sickness, postoperative opioid use, and a history of PONV) (2).
Untreated, PONV occurs in about 30% of the general surgical population and in up to 70-80% of high-risk surgical patients (3-5). The adverse effects of PONV range from patient-related distress to postoperative morbidity. PONV associated with ambulatory surgery increases health care costs due to hospital admission and accounts for 0.1-0.2% of these unanticipated admissions and PONV in nonambulatory surgery may contribute to increased costs, increased length of stay, increased perioperative morbidity and prolonged overall recovery.
Tools for assessing the risk of postoperative nausea/vomiting
Six popular predictive models for PONV have been developed (4,6-10). These models were compared with respect to validity (discriminating power and calibration characteristics) and practicability. Apfel and colleagues analyzed and compared these and found that the simplified risk scores provided better discrimination and calibration properties compared with the more complex risk scores (11).
The incidence of postoperative nausea and vomiting (PONV) still appears to be about 30% (2,12,13). The cost of prophylactic treatment may be contained by keeping the number of patients needed to be treated small through the use of a multimodal approach for identifying patients at high risk (14).
Pierre et al. examined the simplified Apfel score that considers four risk factors: female gender, previous history of PONV or motion sickness, non-smoking status and postoperative use of opioids (Apfel-score). A previously published score includes, in addition to these factors, duration, type of anesthesia and surgery (Sinclair-score). The simplified 4-item Apfel-score presented with favorable discriminating and calibration properties for predicting the risk of PONV (Table 1) (15).
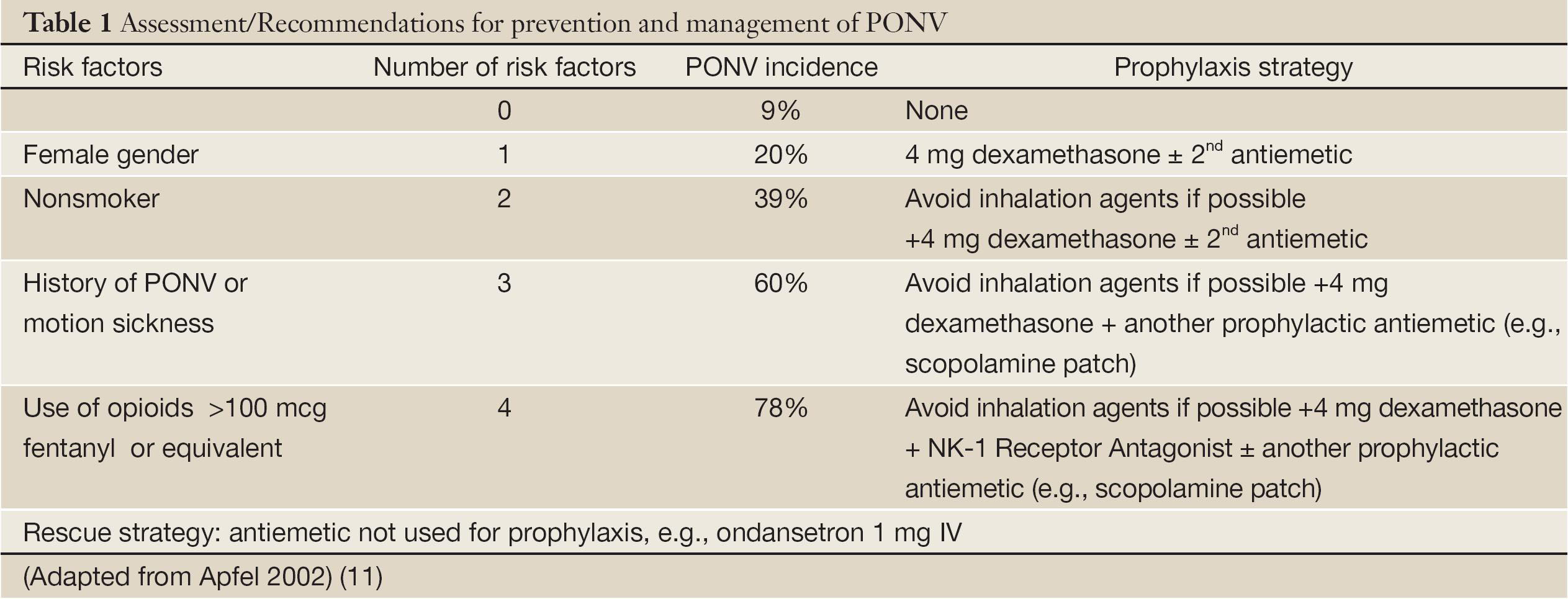
Full table
Sarin and colleagues attempted to develop a better model to predict the patient’s risk for PONV by incorporating both non-modifiable patient characteristics and modifiable practitioner-specific anesthetic practices (16). Their experimental model (EM) was compared against the original Apfel model (OAM), refitted Apfel model (RAM), simplified Apfel risk score (SARS), and refitted Sinclair model (RSM) by examining the discriminating power calculated using area under the curve (AUC) and by examining calibration curves. The EM showed statistically significant improved discrimination over existing models and good calibration. However, the EM should be validated at another institution (16).
The impact of nausea/vomiting
Chancellor and colleagues conducted a two-stage study in France, Germany, Italy, Spain, Sweden, and the United Kingdom of the stated preferences of chronic pain sufferers treated with classic strong opioids and of physicians treating such patients. Sufferers ranked nausea, pain impact, energy, alertness, and constipation; physicians ranked pain response, central nervous system (CNS) effects, nausea, dose form, and constipation in descending order of importance. Sufferers were unwilling to incur severe side effects to decrease pain and chose the opt-out in approximately one half of the choice tasks, whereas physicians were willing to trade between profiles (17).
Macario and colleagues performed surveys of one hundred one patients in the preoperative clinic completed a written survey (18). Patients were asked to rank (order) 10 (nine and one-normal) possible postoperative outcomes from their most undesirable to their least undesirable perioperative outcome. Patients were also asked to distribute $100 among the 10 outcomes, proportionally more money being allocated to the more undesirable outcomes. The dollar allocations were used to determine the relative value of each outcome. Rankings and relative value scores correlated closely (r2=0.69). Patients rated from most undesirable to least undesirable (in order): vomiting, gagging on the tracheal tube, incisional pain, nausea, recall without pain, residual weakness, shivering, sore throat, and somnolence (F-test <0.01) (Table 2) (18).
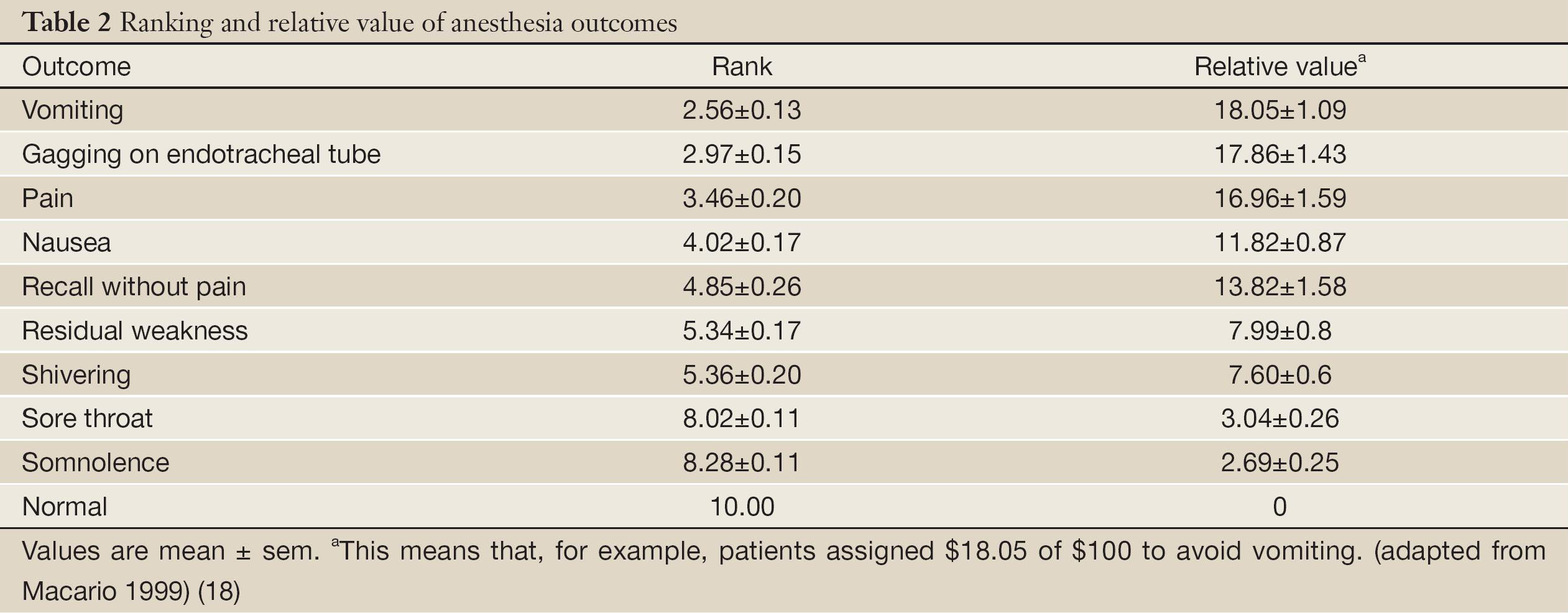
Full table
In 2001, Gan et al. reported that patients associated a value with the avoidance of PONV and were willing to pay between US $56 and US $100 for a hypothetical completely effective antiemetic (19).
Ponv prophylaxis
Prophylaxis is rarely warranted in low-risk patients, moderate-risk patients may benefit from a single intervention, and multiple interventions should be reserved for high-risk patients (Table 2) (5). High-risk patients may require multiple agents for effective PONV prophylaxis. Honarmand and colleagues conducted a randomized, double-blind, placebo-controlled study, in which patients were divided into 4 groups of 20 each and received haloperidol 2 mg i.v. (Group H); midazolam 2 mg i.v. (Group M); haloperidol 2 mg plus midazolam 2 mg i.v. (Group HM); saline i.v. (Group C) (20). Patients in group HM had significantly lower incidence of PONV compared with groups H, M, and C throughout 0-24 h (P<00.5). The HM group had the lowest incidence of PONV (0-2, 2-24, and 0-24 h) and the highest incidence of complete response. Postoperative anti-emetic requirement was significantly less in group HM compared with group M or H (P<0.05) (20).
Pharmacologic treatment strategies for PONV
Kooij and colleagues conducted a prospective study of 2,662 patients (1,681 in the intervention period and 981 in the control period) and found that automated reminders decrease postoperative nausea and vomiting incidence in a general surgical population and improve patient outcome by improving treatment guideline adherence (21).
In selected high-risk populations, the incidence may be as high as 80% (4,22). PONV is the second cause (after pain) for unplanned admission after day-care surgery and can also be a contributing factor to several complications, such as suture dehiscence and aspiration (23,24). A large body of research exists on the evaluation and management of PONV, which has led to the development of risk scores, guidelines, and treatment protocols (5,11,25,26). Kooij revealed that adherence to PONV prophylaxis guidelines to be as low as 37% (27).
In 2006, Carlisle and Stevenson performed a Cochrane Sysetmic Review and published that for 100 people, of whom 30 would vomit or feel sick after surgery if given placebo, 10 people would benefit from a drug and 90 would not. Between one to five patients out of every 100 people may experience a mild side effect, such as sedation or headache, when given an antiemetic drug (25).
NSAIDs (and acetaminophen) reduced postoperative opioid consumption, however, only NSAIDs decreased the incidence of PONV (P<0.05) (28). The enhanced recovery after surgery (ERAS) group recommendations (29) integrated a range of perioperative interventions in order to improve postoperative recovery and enhance hospital discharge.
Postoperative nausea and vomiting (PONV) has been identified as an essential component in achieving patient satisfaction (30) and can be more distressing than pain (19,31). Untreated, one third of patients who undergo surgery will experience PONV, which is associated with prolonged inpatient length of stay (LOS) (32). esophageal rupture, delayed recovery, wound dehiscences and pulmonary complications (e.g., aspiration pneumonia) (5). PONV assessment allows appropriate antiemetic administration. A previous history of PONV, female gender, non-smoking and postoperative opioid administration are the most important predictors of developing PONV (4).
A prospective factorial trial of six placebo controlled interventions/trials (5) preventing PONV included all of the interventions recommended by the ERAS protocol. These included total intravenous anesthesia (TIVA) and the administration of intravenous dexamethasone and ondansetron. Two RCT’s assessed the efficacy of TIVA in reducing the incidence of PONV (5,33). and demonstrated a statistically significant reduction in the immediate incidence of PONV in the TIVA group compared to the traditional anesthesia group. No significant reduction in PONV was observed at 48 or 72 h postoperatively (33). Three RCTs (5,34,35) assessed the efficacy and timing of the administration of intravenous dexamethasone. All trials demonstrated a significant reduction in PONV with dexamethasone compared to placebo. There were no statistically significant differences between the timing of giving steroids at the beginning or end of surgery at 24 h.
Four RCTs (5,36-38) assessed the efficacy and timing of 5-HT3 antagonist administration in preventing PONV. Three trials (5,37,38) of four RCTs (5,36-38) assessing 5-HT3 antagonists demonstrated a significant improvement in PONV in the treatment group compared to placebo. In one trial (5), the 5-HT3 antagonist was given at the end of surgery, while in the other two trials (37,38). it was given at induction and no signify cant differences were found.
Apfel et al. (5) demonstrated that PONV occurs in 59% of all patients undergoing GA with inhalational agents and nitrous oxide. The use of propofol reduces the risk of PONV by 19% and avoiding nitrous oxide by 12%. Combining propofol and air reduces the risk of PONV by 25% (26).
Current ERAS recommendations advise the use of 5-hydroxytryptamine (5-HT3) receptor antagonists (ondansetron) and steroids (dexamethasone). These antiemetics are currently recommended for patients at moderate to severe risk of PONV. Ondansetron and dexamethasone are equally effective and each independently reduce the risk of PONV by 25% (5).
Schaub and colleagues analyzed 25 trials (2,957 patients) (39). Doses varied from 0.25 to 1.0 mg. For prevention of early nausea (within 6 h postoperatively), relative risk (RR) was 0.45 (95% CI, 0.35 to 0.58); number needed to treat (NNT) was 7, 4, and 2 for low, medium and high baseline risk (i.e., control event rate 25%, 50%, 75%). For prevention of early vomiting, RR was 0.65 (95% CI, 0.57 to 0.74), NNT 11, 6, and 4. For prevention of late nausea (within 24 h), RR was 0.74 (95% CI, 0.62 to 0.87), NNT 15, 8, and 5. For prevention of late vomiting, RR was 0.61 (95% CI, 0.47 to 0.80), NNT 10, 5, and 3. Droperidol decreased the risk of headache but increased the risk of restlessness (39).
The glucocorticoid receptors exist in the part of the brain stem where the nucleus of solitary tract and area postrema reside (40). Recent animal experiments have proved that glucocorticoid receptors on both sides of the nucleus of the solitary tract, not area postrema, in the brain stem act to conduct the main antiemetic effect of dexamethasone (41-43). Other possible explanations for dexamethasone preventing PONV include central inhibition of prostaglandin synthesis, reduction of central serotonin activity, and change of permeability of blood-brain barrier to plasma proteins (44).
In December 2001, the U.S. Food and Drug Administration issued a black box warning, stating that the use of droperidol (butyrophenone class of drugs) may be related to fatal arrhythmia (torsade de pointes) (45). However, a combination of dexamethasone and serotonin antagonist appears to address both early and late nausea/ emesis and thus, may be the most effective treatment of preventing PONV (46).
Chen and colleagues performed a meta-analysis of randomized controlled trials of a single dose of dexamethasone (8 mg) for prevention of postoperative nausea and vomiting in patients undergoing thyroidectomy (47). Five RCTs were included with a total of 497 patients. A statistically and clinically significant difference in the incidence of PONV was found in favor of dexamethasone [relative risk (RR) 0.38; 95% confidence interval (CI), 0.30-0.49]. No steroidrelated complications were noted (47).
Wu and colleagues performed a systemic review and meta-analysis of efficacy of ondansetron vs. metoclopramide in prophylaxis of postoperative nausea and vomiting after laparoscopic cholecystectomy. The total incidence of postoperative nausea and vomiting within 24 hours after laparoscopic cholecystectomy was 31% (74 of 235) in the ondansetron group and 56% (127 of 225) in the metoclopramide group (OR=0.33, 95% CI, 0.22-0.49, P<0.00001, I2=49%) (48). Thus, it appears that ondansetron has a better effect than metoclopramide for preventing postoperative nausea and vomiting after laparoscopic cholecystectomy (48).
In this systematic review and meta-analysis, transdermal scopolamine (TDS) was associated with significant reductions in PONV with both early and late patch application during the first 24 hours after the start of anesthesia. TDS was associated with a higher prevalence of visual disturbances at 24 to 48 hours after surgery, but no other AEs, compared with placebo (49).
Gan et al. conducted a randomized, double-blinded study of transdermal scopolamine used as prophylaxis for PONV compared combination therapy (4 mg IV ondansetron plus transdermal scopolamine patch) to ondansetron alone (4 mg IV) in 620 adult females considered at risk for PONV (50) in patients undergoing either outpatient laparoscopy or breast augmentation surgery. The study was placebo controlled, in that some patients received a sham patch. Patients were assessed at 24 and 48 hours for PONV. The combination therapy of transdermal scopolamine and ondansetron significantly reduced nausea and vomiting/retching compared to ondansetron alone at 24 hours postsurgery. More patients in the combination group than the ondansetron-only group did not experience vomiting or retching and did not use rescue medication (48% versus 39%, P<0.02). The number of patients who had no nausea, no vomiting/retching, and no rescue medication was also significantly greater in the combination therapy group compared to the ondansetrononly group (35% versus 25%, P<0.01). The combination group had a significantly longer time to first episode of nausea, vomiting/retching, or rescue medication compared to the ondansetron-only group (P<0.05). In addition, the cumulative incidence of adverse events was significantly lower in the transdermal scopolamine plus ondansetron group compared to the ondansetron-only group (36.7% versus 49%, P<0.01) (51).
Singhal and colleagues performed a meta-analysis in efforts to compare the efficacy of 5HT3 antagonists against all non-5HT3 antagonism-based pharmacological approaches as a preemptive strategy for PONV in women undergoing breast surgery (52). Nineteen trials were included. All trials were of good methodological quality (Jadad score >3). 5HT3 antagonists are superior to other pharmacological interventions for the prevention of PONV in patients undergoing breast surgery under general anesthesia (52).
Patients with three copies of the CYP2D6 gene, a genotype consistent with ultrarapid metabolism, or both have an increased incidence of ondansetron failure for the prevention of postoperative vomiting but not nausea (53). Unlike patients with chemotherapy-induced nausea and vomiting, perioperative patients who failed ondansetron prophylaxis did not have a significant response to cross-over dosing with granisetron (54).
Candiotti and colleagues conducted a randomized, double-blind study we assessed the efficacy and safety of three different doses of the 5-HT3 receptor antagonist palonosetron, compared with placebo, on the incidence and severity of postoperative nausea and vomiting (PONV) for 72 h postsurgery (55). Patients with > or =2 PONV risk factors were eligible and randomized to receive one of three doses of IV palonosetron (0.025, 0.050, or 0.075 mg) or placebo immediately prior to induction of anesthesia. A single 0.075-mg IV dose of palonosetron significantly increased the CR rate (no emetic episodes and no rescue medication) from 0 to 24 h, decreased nausea severity and patients experienced significantly less interference in their postoperative function due to PONV (55).
NK1 receptor antagonists in PONV
In a randomized, multicentre, double-blind phase III trial, 922 patients undergoing open abdominal surgery were allocated randomly to receive one of the three antiemetic treatments 3 hours or less before the operation: oral aprepitant 40 mg, oral prepitant 125 mg, or i.v. ondansetron 4 mg, or matching placebos for the prevention of PONV (56).
Aprepitant was significantly more effective than ondansetron for preventing vomiting at 24 h (percentage of patients with no vomiting 84%, 86%, and 71%, respectively, in the aprepitant 40 mg, aprepitant 125 mg, and ondansetron groups); and at 48 h post-surgery (percentage of patients with no vomiting 82%, 85%, and 66%, respectively, in the aprepitant 40 mg, aprepitant 125 mg, and ondansetron groups); and in reducing nausea severity in the first 48 postoperative hours (56). The most commonly reported adverse events were pyrexia, constipation, headache, and bradycardia with no differences between the groups.
In another study based on a similar design, aprepitant was superior to ondansetron for prevention of vomiting in the first 24 and 48 h, but no significant differences were observed between aprepitant and ondansetron for nausea control, use of rescue antiemetic, or complete response (57).
A post hoc analysis of the pooled data from these two randomized active-controlled trials was performed on 541 patients in the aprepitant 40 mg group, 532 patients in the aprepitant 125 mg group, and 526 patients in the ondansetron group, in a modified intention-to-treat analysis This analysis showed that in the 24 h after surgery, aprepitant 40 mg was more effective than ondansetron (58).
Although not indicated for PONV, an i.v. form (fosaprepitant) [a prodrug of aprepitant], may be conceivably used for treatment of established PONV. Other NK-1 receptor antagonists at various stages of veleopment include: GR205171 (vofopitant, GlaxoSmithKline), CP-122721 (Pfizer), CJ-11974 (Pfizer), casopitant (GlaxoSmithKline), maropitant (Pfizer), netupitant (Helsinn Healthcare), rolapitant or SCH 619734 (Schering-Plough), T 2328 (Mitsubishi Tanabe Pharma), and vestipitant (GlaxoSmithKline) (59).
The dose of aprepitant for PONV prophylaxis is 40 mg administered 3 hours or less prior to surgery. Aprepitant, effectively diminishes post-operative nausea and vomiting while increasing analgesic tolerance in laparoscopic gynecological procedures (60).
It appears conceivable that at least in certain circumstances NK-1 receptor antagonists and 5-HTRAs may be somewhat synergistic (61,62).
Nonpharmacologic treatment strategies for PONV
Apfel and colleagues performed a literature search and included prospective randomized controlled trials that reported PONV event rates in patients receiving supplemental i.v. crystalloids or a conservative fluid regimen after elective surgery under general anesthesia (63). Supplemental i.v. crystalloids were associated with a lower incidence of overall PONV and several PONV outcomes such as reduced need for antiemetic rescue treatment (63).
Holmér Pettersson and Wengström performed a systematic review of acupuncture prior to surgery to minimize postoperative nausea and vomiting and concluded that all kinds of acupuncture point stimulation, both noninvasive and invasive, seem to prevent PONV with minimal side effects (64).
Summary
Postoperative nausea and vomiting is a distressing symptom that may increase medical costs and delay discharge and recovery. Multiple tools exist to stratify patients according to their risk of developing PONV. Additionally, multiple PONV treatment guidelines exist to help health care providers a general PONV management “road-map”. Although these tools exist, it appears that they are not commonly used in routine clinical practice and also it appears that no uniform to standardized approaches are utilized to evaluate and manage PONV in routine clinical practice.
Acknowledgements
The author would like to thank Pya Seidner for her enormous assistance in the preparation of this manuscript.
Disclosure: The authors declare no conflict of interest.
References
- Gan TJ, Meyer T, Apfel CC, et al. Consensus guidelines for managing postoperative nausea and vomiting. Anesth Analg 2003;97:62-71.
- Roberts SM, Bezinover DS, Janicki PK. Reappraisal of the role of dolasetron in prevention and treatment of nausea and vomiting associated with surgery or chemotherapy. Cancer Manag Res 2012;4:67-73.
- Tramèr MR. A rational approach to the control of postoperative nausea and vomiting: evidence from systemic reviews. Part I. Efficacy and harm of antiemetic interventions, and methodological issues. Acta Anaesthesiol Scand 2001;45:4-13.
- Apfel CC, Läärä E, Koivuranta M, et al. A simplified risk score for predicting postoperative nausea and vomiting. Anesthesiology 1999;91:693-700.
- Apfel CC, Korttila K, Abdalla M, et al. IMPACT Investigators. A factorial trial of six interventions for the prevention of postoperative nausea and vomiting. N Engl J Med 2004;350:2441-51.
- Palazzo M, Evans R. Logistic regression analysis of fixed patient factors for postoperative sickness: a model for risk assessment. Br J Anaesth 1993;70:135-40.
- Koivuranta M, Läärä E, Snåre L, et al. A survey of postoperative nausea and vomiting. Anaesthesia 1997;52:443-9.
- Sinclair DR, Chung F, Mezei G. Can postoperative nausea and vomiting be predicted? Anesthesiology 1999;91:109-18.
- Gan TJ. Current controversies in the management of PONV. In: Sugarman M, Gan TJ, Levy JH, et al, eds. Advances in Anesthesia Research and Patient Management, Vol. 74. Honolulu, HI: International Anesthesia Research Society, 2000:2-5.
- Scholz J, Hennes HJ, Bardenheuer HJ, et al. Postoperative nausea and vomiting—incidence, prophylaxis and therapy. In: Purschke R, ed. Refresher course: current knowledge for anaesthesiologists. Deutsche Akademie für Anästhesiologische Fortbildung 26. Berlin: Springer Verlag, 2000:173-81.
- Apfel CC, Kranke P, Eberhart LH, et al. Comparison of predictive models for postoperative nausea and vomiting. Br J Anaesth 2002;88:234-40.
- Cohen MM, Duncan PG, DeBoer DP, et al. The postoperative interview: assessing risk factors for nausea and vomiting. Anesth Analg 1994;78:7-16.
- Kovac AL. Prevention and treatment of postoperative nausea and vomiting. Drugs 2000;59:213-43.
- Scuderi PE, James RL, Harris L, et al. Multimodal antiemetic management prevents early postoperative vomiting after outpatient laparoscopy. Anesth Analg 2000;91:1408-14.
- Pierre S, Benais H, Pouymayou J. Apfel’s simplified score may favourably predict the risk of postoperative nausea and vomiting. Can J Anaesth 2002;49:237-42.
- Sarin P, Urman RD, Ohno-Machado L. An improved model for predicting postoperative nausea and vomiting in ambulatory surgery patients using physician-modifiable risk factors. J Am Med Inform Assoc 2012. [Epub ahead of print].
- Chancellor J, Martin M, Liedgens H, et al. Stated preferences of physicians and chronic pain sufferers in the use of classic strong opioids. Value Health 2012;15:106-17.
- Macario A, Weinger M, Carney S, et al. Which clinical anesthesia outcomes are important to avoid? The perspective of patients. Anesth Analg 1999;89:652-8.
- Gan T, Sloan F, Dear Gde L, et al. How much are patients willing to pay to avoid postoperative nausea and vomiting? Anesth Analg 2001;92:393-400.
- Honarmand A, Safavi M, Khalili G, et al. Prophylactic administration of haloperidol plus midazolam reduces postoperative nausea and vomiting better than using each drug alone in patients undergoing middle ear surgery. Saudi J Anaesth 2012;6:145-51.
- Kooij FO, Vos N, Siebenga P, et al. Automated reminders decrease postoperative nausea and vomiting incidence in a general surgical population. Br J Anaesth 2012;108:961-5.
- Koivuranta M, Laara E. A survey of postoperative nausea and vomiting. Anaesthesia 1998;53:413-4.
- Junger A, Klasen J, Benson M, et al. Factors determining length of stay of surgical day-case patients. Eur J Anaesthesiol 2001;18:314-21.
- Macario A, Weinger M, Truong P, et al. Which clinical anesthesia outcomes are both common and important to avoid? The perspective of a panel of expert anesthesiologists. Anesth Analg 1999;88:1085-91.
- Carlisle JB, Stevenson CA. Drugs for preventing postoperative nausea and vomiting. Cochrane Database Syst Rev 2006;3:CD004125.
- Gan TJ, Meyer TA, Apfel CC, et al. Society for Ambulatory Anesthesia guidelines for the management of postoperative nausea and vomiting. Anesth Analg 2007;105:1615-28.
- Kooij FO, Klok T, Hollmann MW, et al. Decision support increases guideline adherence for prescribing postoperative nausea and vomiting prophylaxis. Anesth Analg 2008;106:893-8.
- Rawlinson A, Kitchingham N, Hart C, et al. Mechanisms of reducing postoperative pain, nausea and vomiting: a systematic review of current techniques. Evid Based Med 2012;17:75-80.
- Lassen K, Soop M, Nygren J, et al. Consensus review of optimal perioperative care in colorectal surgery: Enhanced Recovery After Surgery (ERAS) Group recommendations. Arch Surg 2009;144:961-9.
- Eberhart LH, Morin AM, Wulf H, et al. Patient preferences for immediate postoperative recovery. Br J Anaesth 2002;89:760-1.
- van den Bosch JE, Bonsel GJ, Moons KG, et al. Effect of postoperative experiences on willingness to pay to avoid postoperative pain, nausea, and vomiting. Anesthesiology 2006;104:1033-9.
- Marret E, Remy C, Bonnet F. Meta-analysis of epidural analgesia versus parenteral opioid analgesia after colorectal surgery. Br J Surg 2007;94:665-73.
- Visser K, Hassink EA, Bonsel GJ, et al. Randomized controlled trial of total intravenous anesthesia with propofol versus inhalation anesthesia with isofluranenitrous oxide: postoperative nausea with vomiting and economic analysis. Anesthesiology 2001;95:616-26.
- Wang JJ, Ho ST, Tzeng JI, et al. The effect of timing of dexamethasone administration on its efficacy as a prophylactic antiemetic for postoperative nausea and vomiting. Anesth Analg 2000;91:136-9.
- Feo CV, Sortini D, Ragazzi R, et al. Randomized clinical trial of the effect of preoperative dexamethasone on nausea and vomiting after laparoscopic cholecystectomy. Br J Surg 2006;93:295-9.
- Sun R, Klein KW, White PF. The effect of timing of ondansetron administration in outpatients undergoing otolaryngologic surgery. Anesth Analg 1997;84:331-6.
- Liberman MA, Howe S, Lane M. Ondansetron versus placebo for prophylaxis of nausea and vomiting in patients undergoing ambulatory laparoscopic cholecystectomy. Am J Surg 2000;179:60-2.
- Helmy SA. Prophylactic anti-emetic efficacy of ondansetron in laparoscopic cholecystectomy under total intravenous anaesthesia. A randomised, double-blind comparison with droperidol, metoclopramide and placebo. Anaesthesia 1999;54:266-71.
- Schaub I, Lysakowski C, Elia N, et al. Low-dose droperidol (≤1 mg or ≤15 μg·kg-1) for the prevention of postoperative nausea and vomiting in adults: quantitative systematic review of randomised controlled trials. Eur J Anaesthesiol. 2012;29:286-94.
- Morimoto M, Morita N, Ozawa H, et al. Distribution of glucocorticoid receptor immunoreactivity and mRNA in the rat brain: an immunohistochemical and in situ hybridization study. Neurosci Res 1996;26:235-69.
- Ho CM, Ho ST, Wang JJ, et al. Effects of dexamethasone on emesis in cats sedated with xylazine hydrochloride. Am J Vet Res 2001;62:1218-21.
- Ho CM, Ho ST, Wang JJ, et al. Dexamethasone has a central antiemetic mechanism in decerebrated cats. Anesth Analg 2004;99:734-39.
- Topal A, Gül NY. Effect of dexamethasone, metoclopramide or acepromazine on emesis in cats sedated with xylazine hydrochloride. Acta Vet Brno 2006;75:299-303.
- Henzi I, Walder B, Tramer MR. Dexamethasone for the prevention of postoperative nausea and vomiting: a quantitative systematic review. Anesth Analg 2000;90:186-94.
- Habib AS, Gan TJ. Food and drug administration black box warning on the perioperative use of droperidol: a review of the cases. Anesth Analg 2003;96:1377-9.
- Ho CM, Wu HL, Ho ST, et al. Dexamethasone prevents postoperative nausea and vomiting: benefit versus risk. Acta Anaesthesiol Taiwan 2011;49:100-4.
- Chen CC, Siddiqui FJ, Chen TL, et al. Dexamethasone for prevention of postoperative nausea and vomiting in patients undergoing thyroidectomy: meta-analysis of randomized controlled trials. World J Surg 2012;36:61-8.
- Wu SJ, Xiong XZ, Cheng TY, et al. Efficacy of Ondansetron vs. Metoclopramide in Prophylaxis of Postoperative Nausea and Vomiting after Laparoscopic Cholecystectomy: A Systematic Review and Meta-Analysis. Hepatogastroenterology 2012;59. [Epub ahead of print].
- Apfel CC, Zhang K, George E, et al. Transdermal scopolamine for the prevention of postoperative nausea and vomiting: a systematic review and meta-analysis. Clin Ther 2010;32:1987-2002.
- Gan TJ, Sinha AC, Kovac AL, et al. A randomized, double-blind, multicenter trial comparing transdermal scopolamine plus ondansetron to ondansetron alone for the prevention of postoperative nausea and vomiting in the outpatient setting. Anesthesia and Analgesia 2009;108:1498-504.
- Pergolizzi JV, Raffa R, Taylor R. Prophylaxis of postoperative nausea and vomiting in adolescent patients: a review with emphasis on combination of fixed-dose ondansetron and transdermal scopolamine. J Drug Deliv 2011;2011:426813.
- Singhal AK, Kannan S, Gota VS. 5HT3 antagonists for prophylaxis of postoperative nausea and vomiting in breast surgery: a meta-analysis. J Postgrad Med 2012;58:23-31.
- Candiotti KA, Birnbach DJ, Lubarsky DA, et al. The impact of pharmacogenomics on postoperative nausea and vomiting: do CYP2D6 allele copy number and polymorphisms affect the success or failure of ondansetron prophylaxis? Anesthesiology 2005;102:543-9.
- Candiotti KA, Nhuch F, Kamat A, et al. Granisetron versus ondansetron treatment for breakthrough postoperative nausea and vomiting after prophylactic ondansetron failure: a pilot study. Anesth Analg 2007;104:1370-3.
- Candiotti KA, Kovac AL, Melson TI, et al. A randomized, double-blind study to evaluate the efficacy and safety of three different doses of palonosetron versus placebo for preventing postoperative nausea and vomiting. Anesth Analg 2008;107:445-51.
- Diemunsch P, Gan TJ, Philip BK, et al. Singledose aprepitant vs ondansetron for the prevention of postoperative nausea and vomiting: a randomized, double-blind Phase III trial in patients undergoing open abdominal surgery. Br J Anaesth 2007;99:202-11.
- Gan TJ, Apfel CC, Kovac A, et al. A randomized, doubleblind comparison of the NK1 antagonist, aprepitant, versus ondansetron for the prevention of postoperative nausea and vomiting. Anesth Analg 2007;104:1082-9.
- Diemunsch P, Apfel C, Gan TJ, et al. Preventing postoperative nausea and vomiting: post hoc analysis of pooled data from two randomized active-controlled trials of aprepitant. Curr Med Res Opin 2007;23:2559-65.
- Diemunsch P, Joshi GP, Brichant JF. Neurokinin-1 receptor antagonists in the prevention of postoperative nausea and vomiting. Br J Anaesth 2009;103:7-13.
- Kakuta N, Tsutsumi YM, Horikawa YT, et al. Neurokinin-1 receptor antagonism, aprepitant, effectively diminishes post-operative nausea and vomiting while increasing analgesic tolerance in laparoscopic gynecological procedures. J Med Invest 2011;58:246-51.
- Stathis M, Pietra C, Rojas C, et al. Inhibition of substance P-mediated responses in NG108-15 cells by netupitant and palonosetron exhibit synergistic effects. Eur J Pharmacol 2012;689:25-30.
- Altorjay A, Melson T, Chinachoit T, et al. Casopitant and ondansetron for postoperative nausea and vomiting prevention in women at high risk for emesis: a phase 3 study. Arch Surg 2011;146:201-6.
- Apfel CC, Meyer A, Orhan-Sungur M, et al. Supplemental intravenous crystalloids for the prevention of postoperative nausea and vomiting: quantitative review. Br J Anaesth 2012;108:893-902.
- Holmér Pettersson P, Wengström Y. Acupuncture prior to surgery to minimise postoperative nausea and vomiting: a systematic review. J Clin Nurs 2012;21:1799-805.

